Chronische GVHD (cGVHD) is een veelvoorkomende complicatie na allogene stamceltransplantatie. Beschreven incidenties van cGVHD variëren van 6% tot 80%. Variabelen die deze grote variatie verklaren zijn: de leeftijd van de ontvanger, donor type, type hematopoietische stamcellen (PBSC versus beenmerg), transplantaatmanipulatie (T-celdepletie) en post transplantie donor lymfocyten infusie (DLI). Het klinische syndroom van cGVHD lijkt het meest op auto-immuun en andere immunologische ziekten zoals sclerodermie, ziekte van Sjögren, primaire biliaire cirrhose, wasting syndroom, bronchiolitis obliterans, immuun cytopenieën en chronische immuundeficiëntie. De symptomen presenteren zich meestal gedurende de eerste 3 jaar na allogene stamceltransplantatie en worden vooral gezien bij patiënten die ook een acute GVHD hebben gehad. De belangrijkste symptomen waarop men klinisch moet letten zijn: sclerotische huidveranderingen, lichen planusachtige huidafwijkingen, maculopapulaire huidrashesdaenensmg, orale lichen planus of orale ulcera, dysfagie met oesofagusstrictuur, gewichtsverlies, gewrichtscontracturen, obstructieve of restrictieve longafwijkingen.
De pathogenese is beduidend minder gedefinieerd dan bij acute GvHD. Huidige concepten zijn o.a. persisteren van alloreactieve T- cellen, een Th1-Th2 shift van de cellulaire immuunrespons, falen van controle door regulatoire T cellen (Treg) en/of gestoorde negatieve selectie van T-cellen in de thymus, vervanging van antigeenpresenterende cellen van de ontvanger door donor APC, auto- en alloantistofproductie door B-cellen en niet specifieke mechanismen van chronische inflammatie resulterend in fibrose van het aangedane orgaan.
Herhaalde sinusitiden en bronchitiden zijn vaak een uiting van verminderde afweer welke is geassocieerd met cGVHD. Dit kan gepaard gaan met diepe hypogammaglobulinemie.
De mediane duur van cGVHD is ruim 3 jaar. Daarom behoeft cGVHD ook langdurige behandeling. Dit maakt dat het stellen van de juiste diagnose belangrijk is. Wij volgen de diagnostische en stadiëringscriteria zoals die zijn voorgesteld door de NIH consensus werkgroep.
Diagnostische criteria chronische GVHD
(Jagasia et al. Biology of Blood and Marrow Transplantation. 2015:21:389-401)
| Organ or Site | Diagnostic (sufficient to establish the diagnosis of cGVHD) | Distinctive* (seen in cGVHD, but insufficient alone to establish a diagnosis of cGVHD) | Other Features or Unclassifies Entrities† | Common ±(seen with both acute and cGVHD) |
|---|---|---|---|---|
| Skin | Poikiloderma Lichen planus-like features Sclerotic features Morphea-like features Lichen sclerosus-like features |
Depigmentation Papulosquamous lesions |
Sweat impairment Ichthyosis Keratosis pilaris Hypopigmentation Hyperpigmentation |
Erythema Maculopapular rash Pruritus |
| Nails | Dystrophy Longitudinal ridging, splitting, or brittle features Onycholysis Pterygium unguis Nail loss (usually symmetric, affects most nails)# |
|||
| Scalp and body hair | New onset of scarring or nonscarring scalp alopecia (after recovery from chemoradiotherapy) Loss of body hair Scaling |
Thinning scalp hair, typically patchy, coarse, or dull (not explained by endocrine of other causes) Premature gray hair |
||
| Mouth | Lichen planus-like changes | Xerostomia Mucoceles Mucosal atrophy Pseudomembranes |
Gingivitis Mucositis Erythema Pain |
|
| Eyes | New onset dry, gritty, or painful eyes Cicatricial conjunctivitus Keratoconjunctivitus sicca$ Confluent areas of punctate keratopathy |
Photophobia Periorbital hyperpigmentation Blepharitis (erythema of the eyelids with ederma) |
||
| Genitalia
Females Males |
Lichen planus-like features Lichen sclerosus-like features Vaginal scarring or clitoral/labial agglutination Phimosis or urethral/meatus Scarring or stsnosis |
Erosions Fissures Ulcers |
||
| GI tract | Esophageal web Strictures or stenosis in the upper to mid third of the esophagus |
Exocrine pancreatic insufficiency | Anorexia Nausea Vomiting Diarrhea Weight loss Failure to thrive (infants and children) |
|
| Liver | Total bilirubin, alk.phosph. >2 x upper limit of normal ALT >2 x Upper limit of normal |
|||
| Lung | Bronchiolitis obliterans diagnosed with lung biopsy$ | Air trapping and bronchietasis on chest CT | Cryptogenis organizing pneumonia Restrictive lung disease # |
BOOP |
| Muscles, fascia, joints | Fasciitis Joint stiffness or contractures secondary to sclerosi |
Myositis or polymyositis¶ | Edema Muscle cramps Arthralgia or arthritis |
|
| Hematopoietic and Immune |
Thrombocytopenia Eosinophilia Lymphopenia Hypo- or hyper-gammaglobulinemia Autoantibodies (AIHA, ITP) Raynaud’s phenomen |
|||
| Other | Pericardial or pleural effusions Ascites Peripheral neuropathy Nephrotic syndrome Myasthenia gravis Cardiac conduction abnormality or cardiomyopathy |
|||
| ALT indicates alanine aminotransferase; AIHA, autoimmune hemolytic anemia; ITP, idiopathic thrombocytopenic purpura. * In all cases, infection, drug effect, malignancy, or other causes must be excluded. † Can be acknowledged as part of the chronic GVHD manifestations if diagnosis is confirmed. ± Common refers to shared features by both acute and chronic GVHD. $ BOS can be diagnostic for lung chronic GVHD only if distinctive sign or symptom present in another organ (see text). # Pulmonary entities under investigation or unclassified. ¶Diagnosis of chronic GVHD requires biopsy. |
||||
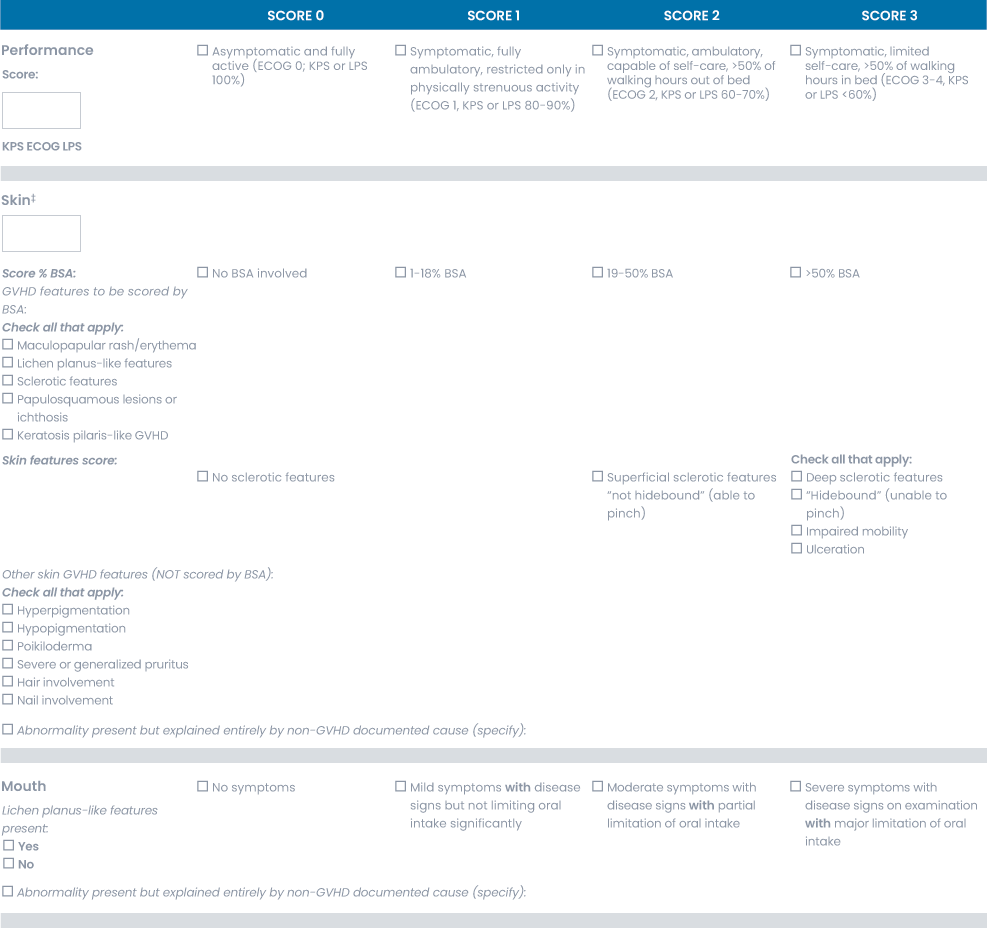
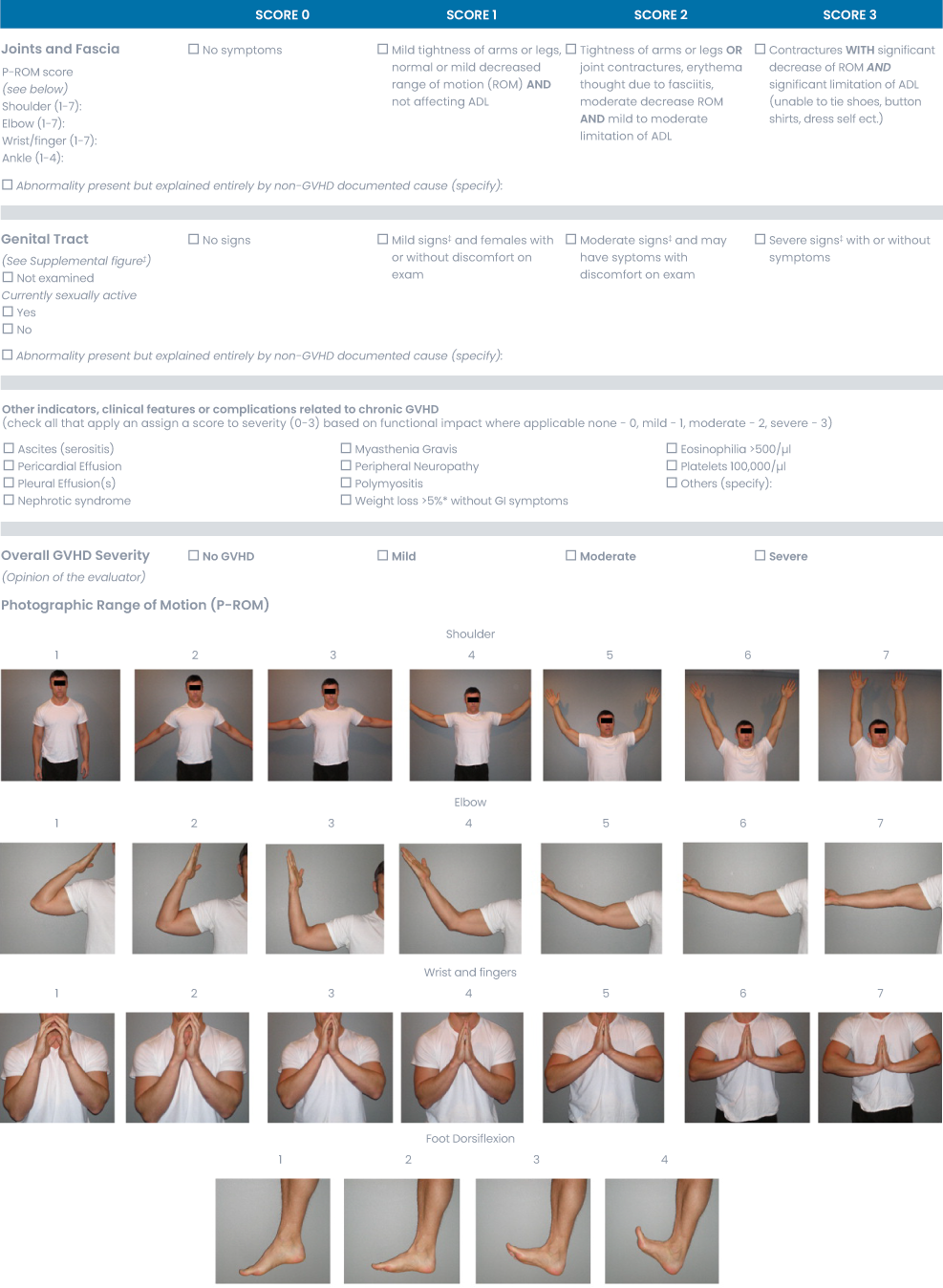
Scoringssysteem chronische GVHD (NIH 2014)
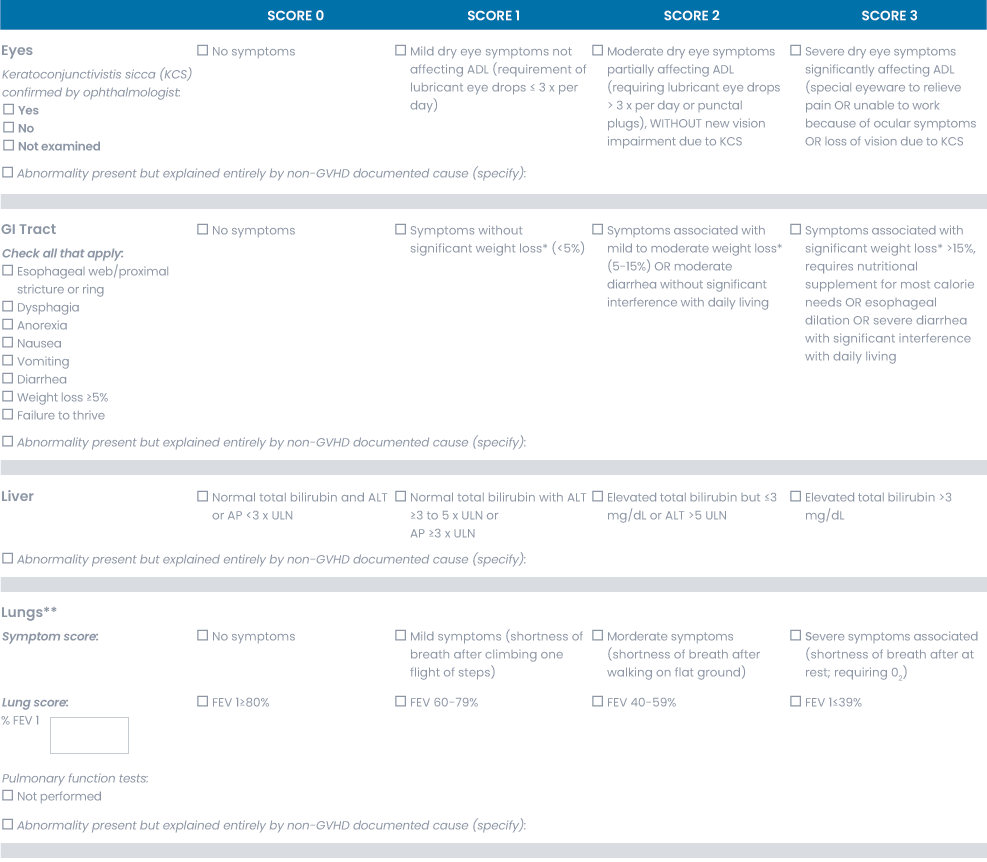
Zie ook scoringsdocument chronische GVHD.
Dit is het scoringssysteem voor cGVHD zoals is voorgesteld door de NIH consensus 2014. Het is belangrijk zich te realiseren dat dit scoringssysteem alleen gebruikt kan worden als er sprake is van cGVHD. Dat wil zeggen als er een diagnostisch criterium is of als er een diagnostische eigenschap (‘feature’) is ondersteund door een histologisch, radiologisch of laboratoriumbewijs.
Er is sprake van milde chronische GVHD als slechts 1 of 2 organen of lokalisaties (behalve longen!) zijn aangedaan, zonder dat er sprake is van functionele beperking. Dit betekent maximale score van 1 in één of meerdere aangedane organen of lokalisaties.
Bij matige chronische GVHD is er tenminste 1 orgaan met klinisch significante GVHD zonder beperkingen (maximum score 2 in een aangedaan orgaan of lokalisatie) of is er sprake van 3 of meer organen of lokalisaties die aangedaan zijn zonder klinisch significante beperkingen (maximum score 1). Een longscore van 1 wordt ook beschouwd als matige cGVHD.
Bij ernstige chronische GVHD is er sprake van ernstige beperking veroorzaakt door cGVHD (score van 3 in een orgaan of lokalisatie). Een longscore van 2 wordt ook beschouwd als ernstige cGVHD.
In tabelvorm ziet bovenstaande er als volgt uit:
| Ernst cGvHD | Aantal organen/locaties aangedaan | Max score in aangedane organen/locaties |
|---|---|---|
| mild | Één of twee (m.u.v. long #) | 1 # |
| matig | Drie of meer | 1 |
| Één of meer | 2 @ | |
| ernstig | Ongeacht aantal | 3 |
# een longscore van 1 wordt als matig cGvHD aangegeven
@ een longscore van 2 of groter wordt als ernstig cGvHD aangegeven
Voor de volledigheid volgen hieronder de originele Seattle criteria voor het indelen van cGVHD:
- Limited
en/of:- gelokaliseerde huid betrokkenheid.
- Leverdysfunctie door cGVHD
- Extensive
of:- gegeneraliseerde huidbetrokkenheid
- gelokaliseerde huidbetrokkenheid en/of leverdysfunctie door cGVHD, in combinatie met:
- leverhistologie: chronische agressieve hepatitis, bridging necrosis of cirrose, of
- oogbetrokkenheid (Schirmer’s test < 5 mm), of
- histologisch bewezen speekselklier- of mondslijmvliesbetrokkenheid, of
- betrokkenheid van een ander orgaan.
Literatuurlijst
- Ferrara JL et al. Graft-versus-host disease. Lancet. 2009;373:1550-61.
- Jagasia MH, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I The 2014 Diagnosis and staging working group report. Biol. Blood and Marrow Transpl. 2015:21:389-401